Psoriasis and chronic allergy

Jelena Tulcina
Echoton Center of Naturalistic Medicine, Kaunas; Center of Naturalistic Medicine, Zverynas, Vilnius
Psoriasis is a chronic inflammatory disease characterized by typical proliferation of epidermal cells, i.e. keratinocytes, with pink-silver papule. Lesion of the joints may complicate the disease (1). Etiology of the disease is not elucidated. However, it is widely accepted that inflammatory, allergic and immune mechanisms may contribute together with genetic predisposition, which is triggered by various stress conditions and risk factors (2). Risk factors include genetic predisposition, racial and regional characteristics, traumas, infections, tobacco smoking, inadequate diet, alcohol consumption and other concominant diseases (3).
Psoriasis is spread globally. It is one of the most prevalent skin diseases and affects 2-3% population worldwide (4). More than 120,000 are diagnosed with psoriasis in Lithuania. Approximately 20,000 of them are in severe disease state. These patients experience side effects and ineffectiveness of the traditional treatment methods. Biological medicines are modern and effective in such cases. However, their use is limited by the high price. In addition, psoriasis patients often have concomitant diseases, such as depression, cardiovascular diseases, obesity or overweight, diabetes mellitus, Crohn’s disease etc. Psoriasis is a disease that most negatively affects life quality.
Exhausted patients often seek for alternative treatment strategies. Attention to the alternative treatment options has been rising during the last years. Patients’ treatment and monitoring data shows that particular diet ingredients may have pronounced effects on psoriasis etiopathogenesis (3). We have not found any studies where systemic nutrition program is applied in combination with intestinal irrigation, specialized hyperbaric oxygen treatment session etc.
Exhausted patients often seek for alternative treatment strategies. Attention to the alternative treatment options has been rising during the last years. Patients’ treatment and monitoring data shows that particular diet ingredients may have pronounced effects on psoriasis etiopathogenesis (3). We have not found any studies where systemic nutrition program is applied in combination with intestinal irrigation, specialized hyperbaric oxygen treatment session etc.
Study subjects
257 patients with psoriasis of varying severity were treated in Echoton Center of Naturalistic Medicine, Kaunas and Zverynas Center of Naturalistic Medicine, Vilnius. These patients have been treated traditionally by dermatologists previously using standard methods and their medical diagnoses were clearly set in the past. Patients were from different parts of the country.
Patients’ distribution according to their gender and psoriasis severity is presented in Table 1.
Patients’ distribution according to their gender and psoriasis severity is presented in Table 1.
Study methods
Each patient was tested for food intolerance (FI), i.e. chronic allergy, for 150 dietary ingredients according to the method of M. Lovendale (5). 10 ml of venous blood was collected and plasma was separated by incubation in room temperature. “Prime test” plate was used for the test. This plate consists of 15 smaller plates with 10 squares in each of them. The squares were filled with concentrated food ingredients. 10 micro litres of plasma were added to each of them and incubated for 40 minutes in room temperature. Reaction was evaluated by means of computerized microscope Moticam 480P (objective 40x0.65). Each plate was evaluated by counting damaged blood cells (lymphocytes) and the individual reaction to each product was assessed. Thus the degree of chronic allergy was determined. If more than 50% of lymphocytes were damaged, the degree of the chronic allergy was determined as III-IV (Figure 1 and 2).
Most of the patients (nearly 90%) received intestinal irrigation by means of Toxygen model BSC-UV, Dotolo Inc, device. Intestinal irrigation was indicated since most of the patients had dysbacteriosis, almost 80% were complaining of chronic constipations and nearly 60% of them had overweight of varying degree or obesity (4, 43, 44).
In order to increase tissue oxygenation, reduce hypoxia symptoms, improve metabolism of the whole body and skin and to speed up the drainage of toxins, specialized hyperbaric oxygen treatment was employed using SOLACE 210 Hyperbaric Chamber.
Most of the patients (nearly 90%) received intestinal irrigation by means of Toxygen model BSC-UV, Dotolo Inc, device. Intestinal irrigation was indicated since most of the patients had dysbacteriosis, almost 80% were complaining of chronic constipations and nearly 60% of them had overweight of varying degree or obesity (4, 43, 44).
In order to increase tissue oxygenation, reduce hypoxia symptoms, improve metabolism of the whole body and skin and to speed up the drainage of toxins, specialized hyperbaric oxygen treatment was employed using SOLACE 210 Hyperbaric Chamber.
Table 1. Degrees of psoriasis severity
|
Gender
|
Severity degree
|
||
|
I
|
II
|
III
|
|
|
Women
|
19 (36.5%)
|
21 (40.4%)
|
12 (23.1%)
|
|
Men
|
5 (20%)
|
14 (56%)
|
6 (24%)
|
The area of skin lesions and the therapeutic effect were graded. Severity of psoriasis was graded as follows: mild psoriasis – up to 3% of the whole body surface (area of 3 palms taken together), moderate psoriasis – 3-10% (area of 3-10 palms), severe psoriasis – more than 10% (4).
Dietary products were chosen and nutritional program drafted according to the food intolerance test results.
Dietary products were chosen and nutritional program drafted according to the food intolerance test results.
Results
Therapeutic effect was evaluated subjectively: by the well-being of patients, changes in skin lesions area, formation of new lesions and regression of the existing ones. Itching and flaking was also estimated.
Positive disease course was detected in 77 patients: skin lesions (papule size, flaking, itching) regressed and overall patients' health was improved (Table 2). The mean age of study patients was 29.5 years. Health state has improved in 52 women (67.5%) and 25 men (32.5%).
Positive disease course was detected in 77 patients: skin lesions (papule size, flaking, itching) regressed and overall patients' health was improved (Table 2). The mean age of study patients was 29.5 years. Health state has improved in 52 women (67.5%) and 25 men (32.5%).
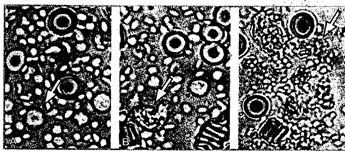 |
Figure 1.
Lymphocyte reaction during the “prime test”. A. – Microscopically normal lymphocytes – no reaction with the pea extract, i.e. extract does not activate the immune system. B. – Chronic immune reaction. Initiation of lymphocyte disintegration. C. – Field full of dead lymphocytes. |
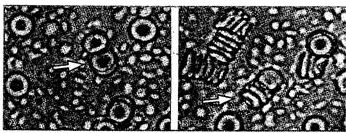 |
Figure 2.
Erythrocyte reaction during the “prime test”. A. – Predominantly normal erythrocytes with agglutination in the center. B. — aggregated erythrocytes that may occlude capillaries and cause organ damage. |
Symptoms in remaining 180 patients have improved by 50-90%. These patients are further treated and monitored.
Women psoriasis was ameliorated after 2.7 months, men — after 2.3 months of monitoring and treatment. Total reduction of psoriasis symptoms was achieved by 4-8 months. During that time patients were strictly following their complex nutritional program, which was updated every month. Patients were recommended to follow the program further and also refine it according to repeated food intolerance (FI) tests. Patients also received colon hydrotherapy (4-5 sessions).
Data obtained proves that clinical improvement of psoriasis symptoms is not always directly associated with the size of skin lesions. It happens that mild psoriasis is much less treatable than a more severe disease.
Women psoriasis was ameliorated after 2.7 months, men — after 2.3 months of monitoring and treatment. Total reduction of psoriasis symptoms was achieved by 4-8 months. During that time patients were strictly following their complex nutritional program, which was updated every month. Patients were recommended to follow the program further and also refine it according to repeated food intolerance (FI) tests. Patients also received colon hydrotherapy (4-5 sessions).
Data obtained proves that clinical improvement of psoriasis symptoms is not always directly associated with the size of skin lesions. It happens that mild psoriasis is much less treatable than a more severe disease.
Five typical psoriasis cases are presented here with the disease history and pictures to better represent the study data. Pictures show that patients had psoriasis of II-III degree. Their nutrition was conventional: meats, breads and milk products were dominant, while the intake of vegetables, fruit and fish was insufficient. Adult patients were consuming coffee, black tea, sweats, sunflower oil, fat of animal origin and other products that were later shown as intolerable by the food intolerance test (FI). All patients received the appropriate number of intestinal irrigations and hyperbaric oxygenation sessions. They all passed food intolerance tests and their individual rotary nutrition programs were composed according to the results of these tests. Nutrition programs were strictly followed.
Skin lesions of psoriasis patients are presented in Figures 3-8.
Discussion
Psoriasis is a complex disease where deep processes of imbalanced organism are reflected in skin lesions. Homeostasis of such an organism depends on nutrition and a psycho-emotional state.
Psoriasis is characterized by proliferation of keratinocytes (1). Epidermal cells of healthy skin are constantly dividing and desquamating from the skin surface. Such a cycle normally lasts 28 days, but in case of psoriasis it accelerates and takes only four days. New cells are forming constantly. Skin is getting thinner. New cells do not maturate and therefore desquamate. Psoriatic skin is red-colored, inflamed, capillaries are dilated and dermal layer is infiltrated with leukocytes (6). Cell proliferation is biochemically controlled by the concentration ratio of two signaling molecules: cAMP and cGMP. While cAMP rises and cGMP decreases, keratinocytes maturates and proliferates less (7). It is reported that in psoriatic skin cGMP concentration is increased. When healthy skin is compared to fully formed flakes, the cGMP concentration is found significantly increased and cAMP decreased (7).
Psoriasis is characterized by proliferation of keratinocytes (1). Epidermal cells of healthy skin are constantly dividing and desquamating from the skin surface. Such a cycle normally lasts 28 days, but in case of psoriasis it accelerates and takes only four days. New cells are forming constantly. Skin is getting thinner. New cells do not maturate and therefore desquamate. Psoriatic skin is red-colored, inflamed, capillaries are dilated and dermal layer is infiltrated with leukocytes (6). Cell proliferation is biochemically controlled by the concentration ratio of two signaling molecules: cAMP and cGMP. While cAMP rises and cGMP decreases, keratinocytes maturates and proliferates less (7). It is reported that in psoriatic skin cGMP concentration is increased. When healthy skin is compared to fully formed flakes, the cGMP concentration is found significantly increased and cAMP decreased (7).
The improvement of psoriasis symptoms may be associated with the less exogenous protein of animal origin taken into the body (this protein was limited up to only 10% of daily food intake). It was replaced with protein of vegetable or fowl origin. Since proteins are stimulating proliferation of epithelium, their lesser amount in daily food may slow down replication processes in the epithelium.
Proteins often cause allergic reactions. Gastrointestinal tract directs a huge stream of amino acids into the blood stream in these cases. This causes allergic reactions and skin lesions. It should be pointed out that allergic reactions may also be stimulated by dysbacteriosis of varying degree. Therefore intestinal irrigation, adequate nutritional program, elimination of sweats from the diet and use of probiotics may decrease dysbacteriosis symptoms. Immune system is involved in pathogenesis of allergic reactions with inflammatory symptoms. It is shown that gluten (gliadin)-free diet improves psoriasis symptoms in some patients. This justifies the idea that gastrointestinal tract plays a role in disease processes (8). Literature review reveals that gluten-free diet improves function of digestive system, i.e. bloating and diarrhea regresses (9, 10-16). Gluten is found in wheat, rye, barley and oats. In the blood of such patients anti-gluten antibodies IgA and/or IgM are found. This is the usual reaction but not the pseudo-allergy. Since most of our patients had food intolerance reactions to some of the mentioned grains, such products were eliminated from their diet.
It is known that proteins of animal origin may affect protein metabolism and induce production of toxic polyamines under influence of intestinal flora, especially when Candida is prevalent. Intestinal flora is responsible for unused polypeptide cleavage (17, 18, 19). Polyamines are eliminated via skin and urine and this illustrates increased autointoxication (20, 21). Increased permeability of intestinal wall contributes to the autointoxication processes (3). Polyamines formed reduce cAMP synthesis via cell proliferation stimulation (17, 18, 19).
Table 2. Time when improvement of psoriasis symptoms occurred.
|
Gender
|
Number of patients
|
Mean age, years
|
Time to improvement, months
|
|
Women
|
52 (67.5%)
|
27.5
|
2.7
|
|
Men
|
25 (32.5%)
|
61.6
|
2.3
|
It is hypothesized that reduction of exogenous protein intake and decrease of polyamine concentration may lead to cAMP increase and down-regulate cell proliferation and disease symptoms. The theory of autointoxication holds that intestinal endotoxins may reach circulation via permeable intestinal walls and up-regulate cGMP concentration in the skin, which further leads to skin cell proliferation in psoriasis patients (22). Lymphocytes contribute to autointoxication since they release partially inactivated inner content when collapsing (5). When supplementation of food fibers is increased by adding more fresh fruits and vegetables into the diet (this is done in our program), the possibility to decrease endotoxin circulation and cGMP skin concentration emerges. Most of the researchers agree that vegetarian diet rich in fibers supports normal intestinal micro-flora while diet rich in protein of animal origin stimulates bacteria to produce endotoxins (23, 24).
 |
 |
|
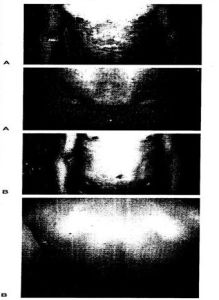
| Figure 3. Patient N.B., age - 30 years, psoriasis history - 15 years. Nobody has psoriasis in the family. Skin lesions: whole body covered with confluent foci, flaking coat on the head, hand skin thick, cracked and bleeding. Nutritional program was composed according to FI test results. Intestinal irrigation and hyperbaric oxygenation sessions were performed. Itching has disappeared and skin condition has improved. A. – Initial state. B. – State after 3 months. |
Figure 4.
Patient M.P., age - 12 years, psoriasis history - 15 month. Disease was aggravated after adenoidectomy when concomitant sepsis was diagnosed and broad spectrum antibiotics administered. Nobody has psoriasis in the family. Skin lesions covered the whole body, skin was flaking and itching. Nutritional program was composed according to FI test results. Intestinal irrigation and hyperbaric oxygenation sessions were performed. Rash has disappeared on the back, abdominal and leg zones after 2 month. Rash on the head disappeared after 6 month. A. – Initial state. B. – State after 6 months. |
Lipid metabolism is also unbalanced in psoriasis. This manifests with incomplete fat acid oxidation, increased lipid peroxidation and lymphokine release. Blood levels of cholesterol, triglycerides, LDL cholesterol and skin- oxidated LDL cholesterol are increased. Free radicals are formed during lipid peroxidation and cause membrane destruction and cell death. All this together activates immune-inflammatory process and skin damage (25).
Oxidative stress is neutralized in keratinocytes by heme oxygenase, which regulates hemoglobin cleavage into biliverdin, Fe and CO. It was reported that heme oxygenase-1 is stress-inducible protein induced by oxidants. It exerts cytoprotective, anti-oxidative and anti-inflammatory properties. Hemoxigenase-1 concentration is found increased in psoriatic skin (26).
According to the results of FI tests our patients received no fat of animal origin, pork, beef or milk products. This was based on the data that free radicals generated from such products would cause oxidative stress, destroy proteins, ribosomes, membranes, specific lipids and DNA (27). Balance between oxidants and anti-oxidants is perturbed in psoriasis patients and lipid peroxidation dominates (28).
FI results were used to determine proper diet oils. Raps, rice, olive, corn and flax-seed oils composed up to 10% of daily calories intake and positively affected clinical symptoms. It is reported that formation of arachidonic acid and malondialdehyde is reduced by fish oil (29). Oils mentioned above have omega-3 polyunsaturated fatty acids (eicosapentaenoic acid and docosahexaenoic acid). It is known that flax-seed and raps oil have omega-3 polyunsaturated fatty acids of 18 carbon molecules which are transformed into 20 carbon molecules containing omega-3 polyunsaturated fatty acids in the body by δ-desaturase. Omega-3 polyunsaturated fatty acids stabilize membranes, regulate their permeability, lower membrane superoxidation, lower hypercholesterolemia, cause vassal dilatation and correct obesity (30). These effects explain the improvement of psoriasis patients’ condition.
 |
Figure 5.
Female patient L.J. Psoriasis history - 6 months. Nobody has psoriasis in the family. Skin lesions covered the whole body, intensive itching and some bleeding sores. Nutritional program was composed according to FI test results. Intestinal irrigation and hyperbaric oxygenation sessions were performed. Following the treatment, skin condition has changed. A. – Initial state. B. – State after 10 months. |
Our data shows that sunflower oil is not suitable since it has higher concentration of omega-6 polyunsaturated fatty acids. Corn oil was used only based on FI test results since it also has omega-6 polyunsaturated fatty acids. This acid is impossible to avoid completely anyway. It is, therefore, crucially important to maintain ratio between omega-3 polyunsaturated fatty acids and omega-6 polyunsaturated fatty acids (1:2-1:8) (30). Arachidonic acid and leucotriens were found increased in psoriatic lesions (31). It was shown that arachidonic acid as well as omega-6 polyunsaturated fatty acids, which are found in products of animal origin, are progenitors of potent inflammation mediators – leucotriens. They are also promoters for cGMP concentration (32, 33). In addition, eicosapentaenoic acid is one of the most active fish oil components – substrates for anti-inflammatory prostaglandins (34). These substances may influence cell proliferation. It is proven that fish oil improves symptoms in mild and moderate psoriasis (33, 35-37). On the other hand, according to some studies fish oil is not superior to raps or olive oil (38).
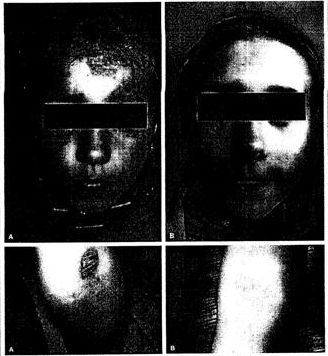 |
Figure 7.
Female patient G.V. Psoriasis history - 12 months. Mother has psoriasis. Skin lesions covered the whole body and head area. Nutritional program was composed according to FI test results. Intestinal irrigation and hyperbaric oxygenation sessions were performed. Following the treatment, skin condition has changed. A. – Initial state. B. – State after 5 months. |
Consumption of tea and herbal extracts may aggravate inflammatory conditions. Yellow safflower (Carthamus tinctorius) exerts anti-inflammatory properties (39, 40) and has an immunomodulatory effect (41). Slippery elm (Ulmus fulva) tea is used in diseases of gastrointestinal tract, stomach and intestinal ulcers as well as colitis. It protects mucous membranes, has herbal mucus, deceases pain and down-regulates inflammation (42). Our patients were recommended to use fruit, rosehip and mint teas. Water with lemon juice, selected according to FI test, was also recommended where possible.
Figure 8.
Female patient A.S. Age – 9 years. Psoriasis history - 7 years. Skin lesions have started in the back of the head hairy area and then have spread onto the back and legs. Skin was itchy, flaky and sometimes bleeding. Nobody has psoriasis in the family. Nutritional program was composed according to FI test results. Intestinal irrigation and hyperbaric oxygenation sessions were performed. Following the treatment, skin condition has changed. A. – Initial state. B. – State after 4 months.
Female patient A.S. Age – 9 years. Psoriasis history - 7 years. Skin lesions have started in the back of the head hairy area and then have spread onto the back and legs. Skin was itchy, flaky and sometimes bleeding. Nobody has psoriasis in the family. Nutritional program was composed according to FI test results. Intestinal irrigation and hyperbaric oxygenation sessions were performed. Following the treatment, skin condition has changed. A. – Initial state. B. – State after 4 months.
Elimination of alcohol consumption is the very important aspect of the diet. Ethanol is a known etiologic factor for psoriasis exacerbation. Although the mechanisms are not clearly elucidated, it is known that ethanol induces hepatic stress and increases permeability of intestinal walls and also serves as the biggest reservoir for free radicals in the body. Hemodialysis procedures are effective for psoriasis patients. This proves that endotoxins, immune complexes and other biologically active substances released during immune reactions are accumulating in the blood. Thus, alcohol consumption does not contribute to the psoriasis treatment strategy.
Literature review reveals that the development of the majority of diseases is associated with function of intestinal system. Food industry has changed its production technologies and food has become more refined and with less ballast fibers. Such food causes intestinal constipation in majority of cases. People may carry up to few kilograms of toxins and other waste material in their intestines. Polluted intestines not only cause the weight gain, but also constantly contaminate body systems with toxins released into the circulation. Helminthes and other parasites are well accommodated in polluted intestines. Intestinal walls overgrown with faeces are not able to adsorb alimentary material effectively and intestinal immune system is depressed. Dysbacteriosis may develop. There are several indications established for colon hydro-therapy, such as constipation or diarrhea, bloating, skin rash up to psoriasis, headache, prostate inflammation and genital discharge (3, 43, 44).
There are reports proving that autointoxication is activated in psoriasis patients and intestines are more permeable. Therefore, endotoxins formed may enter the circulation. Gastrointestinal tract is not cleansed properly. Thus, colon irrigation applied in our study might have helped detoxication and toxic material drainage. The results of this therapeutic procedure combined with diet selected according to the Food Intolerance test has led to a significant psoriasis improvement, i.e. disappearance of skin itching, flaking, skin color normalization and reduced area of skin lesions.
Data presented here proves that complex nutritional program and improved patients’ life style may help to achieve promising results in the diagnosis and management of this complicated skin disease. Based on preliminary results from our correctional study, we may further improve nutritional program that would ultimately reduce psoriasis symptoms and make patients’ life quality even better.
Conclusions
- Psoriasis patients consisted of 67.5% women (mean age 27.5 years) and 32.5% men (mean age 31.6 years).
- More women (63.5%) were experiencing severe psoriasis, i.e. of II and III degree. This number was 20% among men.
- Improvement of psoriasis skin state, i.e. disappearance of skin itching, flaking, skin color normalization and reduced area of skin lesions was detected in women after 2.7 months and in men – after 2.3 months.
- Complex nutritional program and an improved life style may help to achieve positive effects in psoriasis treatment.


